Direct laryngoscopy is a routine procedure conducted to visualize the larynx (voice box), to access, evaluate and treat voice problems. Usually, the laryngoscope is placed through the mouth and the larynx is exposed under general anesthesia without difficulty.
Laryngeal surgeries with the help of an operating microscope (Microlaryngoscopy / MLS) are then conducted to remove the pathology like vocal cord nodule, polyp, etc. The key to successful micro-laryngoscopy is proper laryngeal exposure or visualization of the larynx and laryngeal inlet.
When it comes to the treatment of laryngeal cancers, Transoral laser microsurgery (TLM) is an effective therapeutic approach for early and selected intermediate glottic cancers. Extend of laryngeal exposure is a key limiting factor in determining the feasibility of TLM. If adequate visualization of the entire lesion to be removed is not possible, then curative resection via TLM is not feasible and open procedures should be considered.
In the field of anesthesia, good visualization of the airway is the crucial thing needed for safe and correct tracheal intubation. Poor visualization of the larynx can lead to difficult and traumatic tracheal intubation, inadequate ventilation or even esophageal intubation.
Hence assessment of laryngeal exposure is critical prior to MLS, TLM, and tracheal intubation. Three different grading systems are available for grading of laryngeal exposure.
Cormack Lehane grading system and it’s different modifications.
The Cormack and Lehane (CL), the grading system for laryngeal exposure was first described by R.S. Cormack & J. Lehane in 1984 for obstetric anesthesia. It is the most broadly used to describe laryngeal view during direct laryngoscopy.
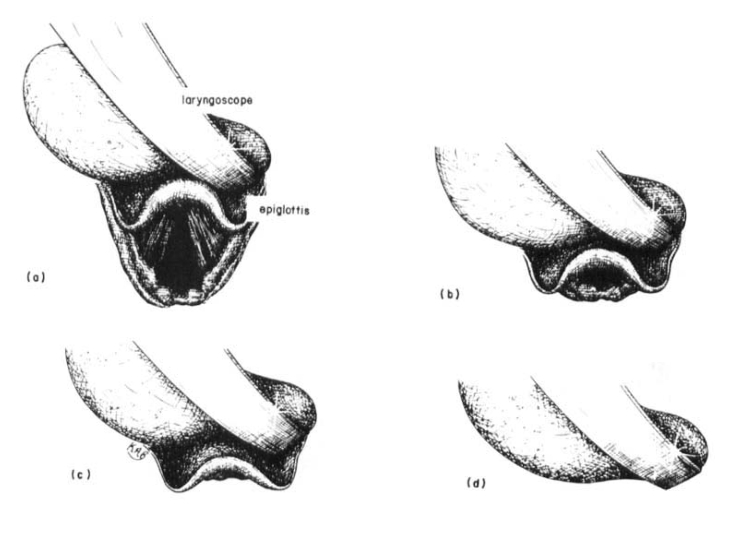
The original Cormack and Lehane, grading system consist of 4 grades as tabulated below.
| Grade 1 | If most of the glottis is visible, then there is no difficulty for intubation. |
| Grade 2 | If only the posterior extremity of the glottis is visible, then there may be a slight difficulty for intubation. Applying light pressure on the larynx will nearly always bring at least the arytenoids into view if not the cords and intubation can be done. |
| Grade 3 | If no part of the glottis can be seen, but only the epiglottis, then there may be fairly severe difficulty for intubation. |
| Grade 4 | If not even the epiglottis can be exposed, then intubation is impossible except by special methods. This situation is well recognized where there is obvious pathology but is exceedingly rare if the anatomy is normal. The epiglottis is the key landmark. If it is not seen withdraw the laryngoscope blade slowly until the epiglottis will drop into view, having previously been in front of the blade. |
Drawbacks of Cormack and Lehane
- Grades are ambiguous between grades 1 and 2, and these grades apply to 95–99% of laryngeal views.
- The discordance between the descriptions and drawings in the original article.
- The descriptive terminology is inexact.
- The variability within grades is so broad as to be meaningless.
- High Intra and inter-observer unreliability.
- Never subjected to rigorous validity testing
Modified Cormack – Lehane Grading System
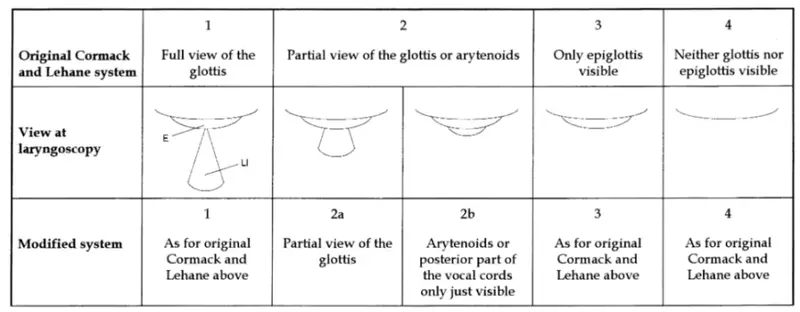
Multiple modifications were made to the CL grading system to overcome its drawbacks. Yentis et al, Wilson et al, Takahata et al all have come up with their own modifications for CL Scoring. Among them, the modification by Yentis et al, in 1998 is mostly accepted. This includes partial views of Grade 2, namely Grade 2a and 2b.
| Grade | Description |
| 1 | Full view of the glottis |
| 2a | Partial view of the glottis |
| 2b | Only posterior extremity of glottis seen or only arytenoid cartilages. |
| 3 | Only epiglottis seen, none of the glottis seen. |
| 4 | Neither glottis nor epiglottis is seen. |
Percentage of Glottic Scoring (POGO) Scoring
To better describe the laryngeal views recorded with an imaging system, Levitan et al in 2002 proposed the percentage of glottic opening (POGO) score. The POGO score essentially provides a continuous, numerical value across the full range of Cormack and Lehane grade.
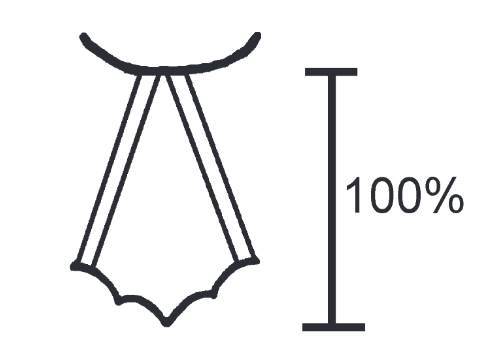
The POGO score represents the percentage of glottic opening seen, defined by the linear span from the anterior commissure to the inter-arytenoid notch.
A POGO score of 100% is a full view of the glottis from the anterior commissure to the inter-arytenoid notch and corresponds to the best CL grade 1 view. A POGO score of 0% means that even the inter-arytenoid notch is not seen, i.e., no portion of the glottis is seen and corresponds to a CL grade 3. A POGO score of 1%, which would include only the inter-arytenoid notch and no other structures, would be the worst CL grade 2 view.
POGO scoring does not provide any differentiation between CL grades 3 and 4 since in each case the POGO score would be zero.
Though POGO scoring showed very good inter and intra-physician reliabilities, which can distinguish various degrees of glottic visualization, this was also not free from drawbacks.
Drawbacks of POGO scoring.
- POGO Score is applied to still images only, not to dynamic video images, which would more closely approximate real condition of laryngeal viewing.
- The validity of the POGO score under the dynamic, real-time conditions of direct laryngoscopy is still pending.
Laryngoscore
In 2014, Piazza et al introduced “Laryngoscore” as clinical predictors of difficult laryngeal exposure for micro-laryngoscopy.
This laryngeal exposure score is based on eleven clinical parameters like interincisors gap (IIG), thyro‐mental distance, upper jaw dental status, trismus, mandibular prognathism, macroglossia, micrognathia, degree of neck flexion‐extension, history of previous open‐neck and/or radiotherapy, Mallampati’s modified score, and body mass index (BMI). Each parameter was assessed to obtain a total score. The minimum score was 0 and the maximum was 17.
Patients were divided into five classes according to the anterior commissure (AC) visualization:
- Class 0, complete AC visualization with large-bore laryngoscopes in the Boyce-Jackson position.
- Class I, as class 0 with external laryngeal counterpressure.
- Class II, as class I in the flexion position.
- Class III, as class II using small-bore laryngoscopes; and
- Class IV, impossible AC visualization
In their study, it was observed that a median score of < 6 corresponds to class 0-I-II (good/acceptable laryngeal exposure). When the Laryngoscore ≥ 6, difficult laryngeal exposure was encountered in 40% and when considering a Laryngoscore of ≥ 9, 67% of patients had a difficult laryngeal exposure.
They concluded that the Laryngoscore is a good predictor of difficult laryngeal exposure and assists in selecting the ideal candidates for operative microlaryngoscopy. A cutoff laryngoscore of 6 distinguishes favorable versus difficult/impossible laryngeal exposures.
References
- & . Difficult tracheal intubation in obstetrics. Anaesthesia 1984; 39: 1105– 11.
- Yentis, S.M.; Lee, D.J. (1998). “Evaluation of an improved scoring system for the grading of direct laryngoscopy”. Anaesthesia. 53 (11): 1041–4.
- Levitan RM, Hollander JE, Ochroch EA. A grading system for direct laryngoscopy. Anaesthesia. 1999 Oct;54(10):1009-10.
- Piazza C, Mangili S, Bon FD, Paderno A, Grazioli P, Barbieri D, Perotti P, Garofolo S, Nicolai P, Peretti G. Preoperative clinical predictors of difficult laryngeal exposure for microlaryngoscopy: the Laryngoscore. The Laryngoscope. 2014 Nov;124(11):2561-7.