Thyroidectomy is a surgical procedure involving removal of the thyroid glands. The procedure can be a hemi-thyroidectomy (partial removal) or can be a total thyroidectomy.
The most important thing about thyroidectomy is the meticulous dissection needed for preserving the two nerves and bilateral parathyroid glands. These two nerves are the Recurrent laryngeal nerve (RLN) and External branch of superior laryngeal nerve (EBSLN).
Knowing the anatomy and landmarks in relation to thyroid helps in preservation of these vital structures during thyroidectomy. Classically multiple triangles are described for identification of these important nerves in thyroidectomy.
In this article we summarize these triangles in relation to thyroidectomy.
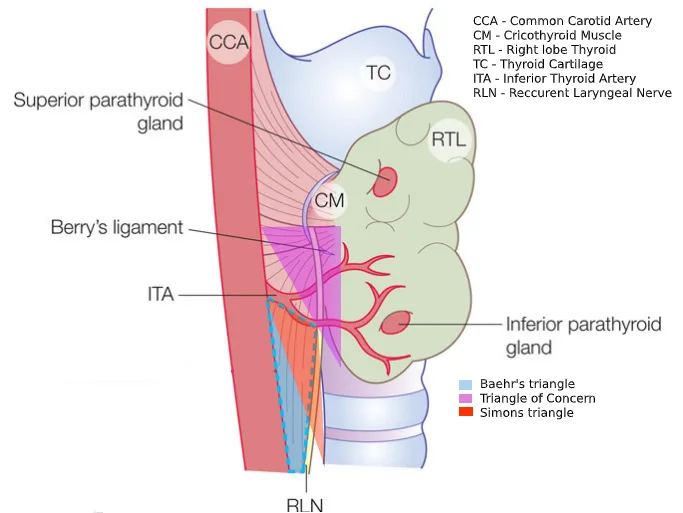
Beahrs Triangle or Riddle’s triangle
This is one of the most important triangles in relation with thyroid. This triangle is named after O H Beahrs. Its synonymous as Riddle’s triangle.
Baehr’s triangle is bounded by
- Base: Common carotid artery
- Superiorly: Inferior thyroid artery
- Medial border: Recurrent laryngeal nerve (RLN)
The triangle lies posterior to the thyroid gland, in the tracheo-esophageal groove.
Boundaries of Baehr’s triangle becomes visible after medial retraction of the thyroid lobe. The inferior thyroid artery crosses the RLN within this triangle, so careful dissection is needed to avoid nerve injury.
Simon’s triangle
Classically, the RLN is identified intraoperatively in Simon’s triangle, which is formed by
- Lateral border: Common carotid artery
- Medial border: Esophagus
- Superior border: Inferior thyroid artery
The inferior thyroid artery often intersects the RLN within this space, requiring careful dissection.
Lore’s Triangle
This triangle described by Lore et al., is also for identification of recurrent laryngeal nerve. This triangle is also known as retrolaryngeal node triangle.
- Medial border: Trachea and Esophagus
- Lateral border: Common Carotid Artery
- Superior border: Inferior Pole of the Thyroid Gland
The RLN is commonly found within this triangle, making it a crucial landmark for nerve preservation. The triangle provides a safe approach to dissecting around the inferior thyroid artery, where the RLN often crosses. Exposure of Lore’s Triangle helps in minimizing nerve injury during thyroidectomy and parathyroidectomy.
RLN triangle
This is an inverted triangle with
- Apex (Inferiorly): Thoracic Inlet, where the RLN emerges from the mediastinum as a single trunk.
- Medial Border: Trachea
- Lateral Border: Medial edge of the retracted strap muscles
- Superior Border: Lower edge of the inferior pole of the thyroid gland
Recurrent laryngeal nerve exits as a single trunk here at thoracic inlet, making it a critical landmark. Identifying the RLN at its thoracic inlet origin ensures safe dissection and reduces the risk of nerve injury. The triangle is particularly useful in cases where the nerve takes an aberrant course or in reoperative thyroid surgeries.
Joll’s Triangle
Joll’s triangle is concerned with identification and preservation of External branch of superior laryngeal nerve (EBSLN).
- The superior border is formed by superior attachment of strap muscles,
- medial border by the midline and
- lateral border formed by the upper pole of thyroid gland and superior thyroid vessels.
EBSLN lies in the floor of the triangle formed by the cricothyroid muscle. The triangle is also named as sternothyroid-laryngeal triangle.
Cricothyroid space of reeves
Reeve’s space is an avascular space between the upper pole of the thyroid gland and the cricothyroid muscle. Identification and opening up of the space is important for preservation of EBSLN.
The space opens up once the medial dissection is performed at the superior pole of thyroid gland. The ipsilateral thyroid lobe is given traction in a downward and outward direction to open up the sternothyroid—laryngeal triangle or “Jolls triangle”.
| Feature | Joll’s Triangle | Cricothyroid Space of Reeves |
|---|---|---|
| Definition | A surgical landmark used to identify and preserve the External Branch of the Superior Laryngeal Nerve (EBSLN) | A fascial space that extends from the cricothyroid muscle to the superior pole of the thyroid gland, where the EBSLN runs |
| Boundaries | Superior: Superior attachment of strap muscles Medial: Midline Lateral: Upper thyroid pole and superior thyroid vessels | Superior: Hyoid bone Inferior: Superior thyroid pole Lateral: Superior thyroid vessels and inferior constrictor muscle |
| Clinical Significance | EBSLN lies in the floor of the triangle, making it an important landmark during thyroidectomy to prevent nerve injury | Important for identifying and preserving the EBSLN as it courses downward towards the cricothyroid muscle |
| Surgical Importance | Helps in safe ligation of superior thyroid vessels without injuring the EBSLN | Provides a fascial plane that allows gentle dissection to locate the EBSLN before ligating vessels |
Triangle of concern
The Triangle of Concern is a crucial anatomical region in thyroidectomy, as it is the most common site for post-operative bleeding and recurrent laryngeal nerve (RLN) injury.
- Medial Border: Trachea
- Lateral Border: Recurrent Laryngeal Nerve (RLN)
- Base: Thyrothymic ligament and loose fat above the sternum
- Apex: Berry’s ligament
This region contains small branches of the inferior thyroid artery, which require careful ligation or cauterization to prevent post-operative hematoma. The RLN runs in close proximity to these small arterial branches, making nerve injury a significant risk. Berry’s ligament at the apex is a critical structure where the RLN is often tethered, requiring precise dissection to prevent nerve traction or transection.
Other landmarks for Recurrent Laryngeal Nerve
In addition to above mentioned triangles, there are some other useful landmarks for RLN. They are
- Inferior thyroid artery (ITA): based on the area of nerve’s crossing with artery. The nerve can be infront / through / behind the artery.
- Right side
- 50% between 2 branches of ITA
- 25% infront of ITA
- 25% behind ITA
- Left side
- 25% between 2 branches of ITA
- 25% infront of ITA
- 50% behind ITA
- At level of upper 2 or 3 tracheal ring, the nerve pierces Berry’s Ligament.
- Wang’s point: A constant landmark for RLN – Laryngeal entry point approximately 1cm below thyroid cartilage’s inferior horn.
- The anterior arch of cricoid is clear landmark and marks the lower edge of cricoid cartilage. Directly lateral is the RLN entry point.
- Tubercle of Zuckerkandl – RLN is just medial to tubercle.
- Right side
References
- Kumar, Prem & Premkumar, Anandan. (2018). The rationale of triangles in relation to thyroid surgery: A proposed unified ‘area of danger’ for safe thyroidectomy. 48. 10.18231/2581-5229.2018.0013.
- Jain, Vikas. (2017). Beahrs’ Triangle: The Surgical Anatomy. World Journal of Endocrine Surgery. 9. 35-35. 10.5005/jp-journals-10002-1206.
- Upile T, Jerjes W, Mahil J, Tailor H, Balakumar R, Rao A, Qureshi Y, Bowman I, Mukhopadhyay S. How to do it: the difficult thyroid. Head & neck oncology. 2011 Dec;3(1):54.