The nasopharynx is an air-containing cavity at the back of the nose, which occupies the uppermost extent of the aerodigestive tract.
It’s like a small cuboidal box about two to three centimeters front to back and about three to four centimeters top to bottom and side to side.
The cavity is lined by pseudostratified ciliated columnar epithelium near the nasal end and non-keratinizing stratified squamous epithelium in the pharyngeal surface.
Boundaries and Communications of nasopharynx
Nasopharynx is bounded,
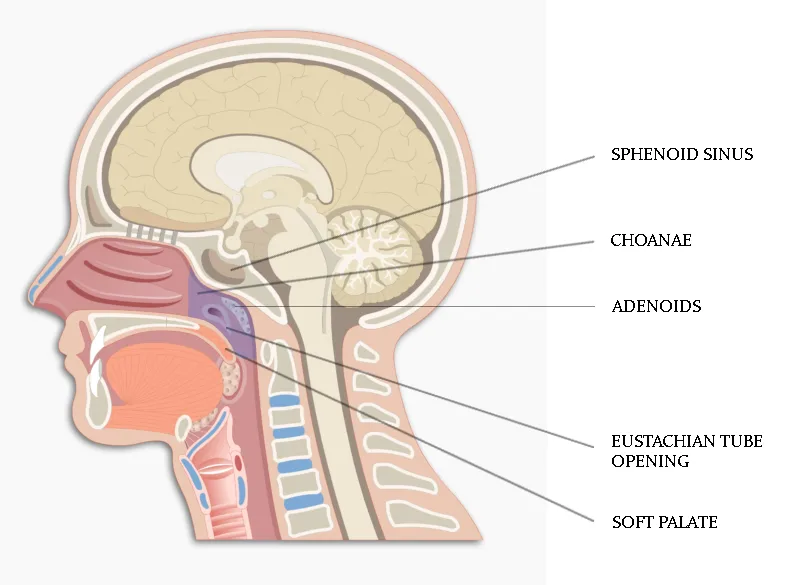
- anteriorly by the posterior end of the nasal septum and the posterior nasal apertures (choanae).
- roof and posterior wall: They imperceptibly merge with each other. It is formed by the sphenoid sinus, the clivus, and anterior aspect of the first two cervical vertebrae.
- the floor is formed by hard palate, the soft palate; and
- lateral nasopharyngeal walls are formed by the margins of the superior constrictor muscle.
Communications of nasopharynx
- Anteriorly, the nasopharynx is in direct continuity with the nasal cavity through the choanae.
- laterally in direct communication with the middle ear cavity through the eustachian tubes and
- inferiorly it communicates with the oropharynx along the posterior border of the soft palate.
Important structures in relation with nasopharynx
Choanae: This is the exit from the nose back into the nasopharynx. There is one on each side from the nose, divided by the nasal septum.
Adenoids / Lymphoid tissue: Adenoids are a subepithelial collection of lymphoid tissue, which is present at the junction of the roof and posterior wall of the nasopharynx. They increase in size up to the age of 6 years and after that gradually atrophies.
Eustachian/Auditory tubes: The Eustachian tubes, lie on each side of the nasopharynx. This tube connects the nasopharynx with the middle ear and helps in equalizing the pressure inside the ears, and in draining mucus from the middle ear.
Torus tubarius: Torus tubarius is the medial cartilaginous extension of the auditory (eustachian) tube which forms a protrusion on the lateral wall of the nasopharynx at the superior and posterior aspects of the opening of the auditory tube.
Tubal tonsil: This collection of subepithelial lymphoid tissue is continuous with adenoid tissue and forms a part of the Waldeyer’s ring. It is situated at the tubal elevation. Enlarged or infected tubal tonsils can block Eustachian tube, leading to hearing problems.
Fossa of Rosenmüller (FOR)/Pharyngeal recess: Just posterior to the torus tubarius lies the pharyngeal fossa, or the fossa of Rosenmüller (FOR). This Fossa of Rosenmüller is formed by the junction of the lateral and posterior walls of the nasopharynx. The fossa can measure up to 1.5 cm in adults.
The importance of FOR is that its a hidden area in regular post nasal examination and is the commonest site of nasopharyngeal carcinoma. Hence it is also called as “Coffin’s corner” – malignancies arising in FOR may go unnoticed and will present in late-stage with poor prognosis. The FOR opens into the nasopharynx at a point below foramen lacerum and is considered as a landmark for carotid artery in endoscopic skull base surgeries.
The important relations of FOR are
- Anteriorly – Eustachian tube and Levator palatini muscle
- Posteriorly – Pharyngeal wall mucosa overlying the pharyngobasilar fascia and retropharyngeal space
- Superiorly – Foramen lacerum and floor of carotid canal.
- Posterolateral or apex – Carotid canal opening and petrous apex posteriorly, foramen ovale and spinosum laterally.
- Medially – Nasopharynx
- Laterally – Tensor palatine and mandibular nerve, prestyloid compartment of parapharyngeal space.
Base of skull: The nasopharynx is located right below and in front of the base of the skull.
Retropharyngeal space: This is a space behind the pharynx, in front of the spine.
Muscles: Pharyngeal constrictor muscles, the levator palatini muscle are two muscles in close relation with the nasopharynx.
Sinus of Morgagni: Sinus of Morgagni is a defect in the lateral pharyngeal wall at the level of nasopharynx, formed due to dehiscence in superior constrictor muscle, which fails to reach the base of the skull. This gap is bridged only by pharyngobasilar fascia.
It is through this opening the eustachian (auditory) tube along with its two muscles enter the nasopharynx. The Ascending palatine artery, which is a branch of the facial artery also runs through this sinus.
As it’s only a membrane-bound region, nasopharyngeal tumors can easily breach this area and spread into the parapharyngeal space.
Rathke’s pouch: This dimple above the adenoids (junction of nasal septum and roof of nasopharynx) is reminiscent of the buccal mucosal invagination, which forms the anterior lobe of the pituitary. A craniopharyngioma may arise from Rathke’s pouch.
Nasopharyngeal bursa: Its an epithelial lined median recess, which is seen within the adenoid mass, extends from pharyngeal mucosa to periosteum of basiocciput. Bursa represents the embryonic site of attachment of notochord to the pharyngeal endoderm.
Tornwaldt’s disease is a abscess that develops in the nasopharyngeal bursa. Infected bursa usually presents with persistent postnasal discharge or crusting.
Passavant’s ridge: This is a mucosal ridge, which encircles the posterior and lateral walls of the nasopharyngeal isthmus, is formed by fibers of palatopharyngeus muscle. When soft palate contracts during deglutition or speech, it makes firm contact with Passavant’s ridge and cut off nasopharynx from the oropharynx.
Nerve supply of nasopharynx
The sensory supply of nasopharynx is by trigeminal (Cranial Nerve V) and Glossopharyngeal nerve (Cranial nerve IX). Anterior to the Eustachian tube, sensory supply is by the second division of trigeminal (Maxillary / V2) nerve while posterior to the tube it’s by the glossopharyngeal nerve.
Motor supply is from the plexus formed by Glossopharyngeal nerve (Cranial nerve IX), Vagus nerve (Cranial Nerve X) and by the sympathetic fibers from the superior cervical ganglion.
Blood supply
The nasopharynx receives its blood supply from Ascending pharyngeal artery, Ascending palatine branch of the facial artery, Ascending cervical artery, Maxillary artery – all are branches of the external carotid artery.
The venous drainage from the superior part is via the pterygoid plexus and from the inferior part via the pharyngeal plexus of veins. All these plexus drains finally into the internal jugular vein.
Lymphatic drainage
Nasopharynx has an extensive lymphatic network system. Lymphatic drainage in the nasopharynx occurs laterally and medially:
- From the posterior wall, the lymphatics drainage is to the retropharyngeal nodes (nodes of Rouviere) and
- from the lateral wall, the lymph vessels traverse the superior constrictor muscle and drain into the lateral retropharyngeal, deep cervical and posterior triangle lymph nodes.
Physiological functions of nasopharynx
Airway: Nasopharynx acts as a conduit for air to its way to the larynx and trachea.
Middle ear ventilation: Eustachian tube ventilates the middle ear and equalizes air pressure on both sides of the tympanic membrane. Dysfunctions of the Eustachian tube can affect middle ear and cause hearing problems.
Resonance: It is a part of the resonating chamber for voice production. Nasopharyngeal obstruction and velopharyngeal incompetence produce changes in voice.
Drainage: It is a drainage channel for nasal and nasopharyngeal mucous secretions.
Nasopharyngeal isthmus: It cuts off nasopharynx from oropharynx during swallowing, vomiting, gagging and speech.