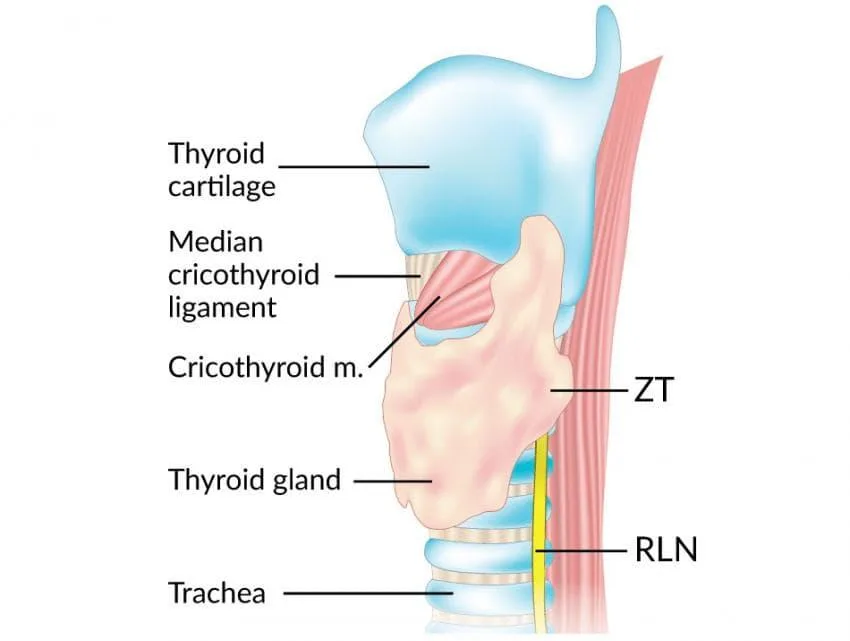
Zuckerkandl Tubercle (ZT) is the posterior projection of lateral lobes of the thyroid gland and is a common anatomical structure observed in 60-90% of cases.
The tubercle was first described by Otto Madelung in 1867 as “posterior horn of the thyroid”. Later in 1902, Emil Zuckerkandl described it as ‘tuberculum’ or ‘processus posterior glandulae thyroideae’.
Gilmour later described the relationship of ZT between recurrent laryngeal nerve (RLN) and superior parathyroid glands.
Anatomy
The thyroid gland develops from the fusion of a median and paired lateral anlagen, arising from two distinct regions of endodermal pharynx, during the first trimester of pregnancy.
Anlagen are the areas of primordial cells which ultimately differentiate into the thyroid follicular cells. The median anlagen involve the midline thyroid tissue extending from the foramen caecum to the level of the larynx along the thyroglossal tract. The two-lateral analgen, also known as ultimobranchial bodies, develop as caudal projections from 4th or 5th pharyngeal pouches. These lateral analgens fuses with median thyroid analgae by 6th week of development forming 10% of the thyroid gland. This point of fusion later forms the Tubercle of Zuckerkandl.
These ultimobranchial bodies produce parafollicular cells / C cells of the thyroid which produces calcitonin, a hormone essential for calcium metabolism in humans.
Zuckerkandl’s tubercle is mostly circular or triangular in shape. It is most commonly located in the middle third of thyroid lobe (in 88% cases), but can be found in the lower part or on the upper third of gland. Various studies have quoted a higher incidence of the tubercle on the right side.
Pelizzo described its anatomical importance as a landmark for recurrent laryngeal nerve during thyroid surgery and classified it into 4 grades.
| Grades | Characteristic | Percentage |
| Grade 0 | Unrecognizable | 0 – 11.25% |
| Grade 1 | Only a thickening of the lateral edge | 20% |
| Grade 2 | Size less than 1cm | 56.25% |
| Grade 3 | Size more than 1 cm | 12.5% |
Clinical significance of tubercle
A landmark for recurrent laryngeal nerve
When present, ZT is considered as a real constant landmark pointing to the RLN during thyroid surgeries. The tubercle indicates the laryngeal entry point of RLN or its anterior branch. The RLN appears to pass through a cleft medial to the tubercle – some surgeons consider this as tubercle covering the entry point of RLN. The tubercle can be above or below this entry point. Careful and meticulous dissection around the tubercle is mandatory for the identification and preservation of the nerve.
In 6% cases, the RLN may be anterior (or lateral) to the tubercle. This is a high-risk situation, placing the nerve at increased risk of damage during dissection.
Relation with parathyroids
The tubercle also separates the superior and inferior parathyroids. The superior parathyroids are seen cranial and posterior to the tubercle while the inferior parathyroids are located caudal and anterior to the tubercle.
Pressure symptoms
Larger tubercle can cause compression at tracheoesophageal groove leading to pressure symptoms like dysphagia.
Recurrence or residual disease
Recognition and removal of the ZT are clearly important for the adequate performance of total thyroidectomy. If not carefully looked for and removed, the tubercle can be a source of persistent, unrelieved symptoms or recurrence after thyroid surgeries.
ZT is also the site for maximum density of C cells, making its resection mandatory in total thyroidectomy for medullary thyroid cancer.
This remnant tissue may be a source of persistent radioiodine uptake on radioactive iodine scans.
Radiology
Radiologically it may be mistaken for a thyroid nodule, mass or lymph node.
Other anatomical structures associated with Zuckerkandl
- Tubercle of Zuckerkandl is a posterolateral projection of the thyroid gland derived from the lateral analgen.
- Concha of Zuckerkandl is a rarely found small nasal concha situated above the supreme nasal concha.
- Zuckerkandl’s dehiscence is small gaps occasionally seen in the layers of the ethmoid bone.
- The organ of Zuckerkandl is a mass of chromaffin tissue found adjacent to the anterior aspect of the aorta, between the inferior mesenteric artery and the aortic bifurcation.
- Zuckerkandl’s fascia is the posterior layer of the renal fascia.
- Zuckerkandl’s gyrus (Zuckerkandl’s convolution) is a thin sheet of grey/white substance in front of, and ventral to, the genu of the corpus callosum.
- Zuckerlandl’s operation is perineal prostatectomy.
References
- Henry BM, Sanna B, Vikse J, Graves MJ, Spulber A, Witkowski C, Tomaszewska IM, Tubbs RS, Tomaszewski KA. Zuckerkandl’s tubercle and its relationship to the recurrent laryngeal nerve: A cadaveric dissection and meta-analysis. Auris Nasus Larynx. 2017 Apr 2.
- Irkorucu O. Zuckerkandl tubercle in thyroid surgery: Is it a reality or a myth?. Annals of Medicine and Surgery. 2016 May 31;7:92-6.
- Sheahan P, Murphy MS. Thyroid tubercle of Zuckerkandl: importance in thyroid surgery. The Laryngoscope. 2011 Nov 1;121(11):2335-7.
- Gurleyik E, Gurleyik G. Incidence and surgical importance of Zuckerkandl’s tubercle of the thyroid and its relations with recurrent laryngeal nerve. ISRN surgery. 2012 Aug 16;2012.