
Tonsils are a pair of small, soft tissue masses located at the back of the throat, one on each side. Scientifically, tonsils are part of the lymphatic system and are classified as secondary lymphoid organs.
The two main types of tonsils are the palatine tonsils, which are the ones commonly referred to as “tonsils,” and the pharyngeal tonsils, also known as the adenoids.
Palatine Tonsils
The palatine tonsils are clusters of lymphatic tissue consisting of lymphocytes, macrophages, and other immune cells. They play a role in the immune system by helping to protect the body against infections. The tonsils contain germinal centers where immune cells are activated and antibodies are produced in response to pathogens, such as bacteria or viruses, that enter the throat.
Anatomy of tonsils
- Palatine tonsils are the largest member of the inner waldeyer’s ring.
- They consist of paired aggregates of lymphoid tissue located in pocket formed between between the anterior (mucosal fold of palatoglossal muscle) and posterior tonsillar pillars (mucosal fold of palatopharyngeal muscle).
- It extends superiorly into the soft palate, inferiorly into the tongue base and anteriorly into palatoglossal arch (formed by palatoglossal muscle).
- Tonsils may be larger in childhood and usually regress in size near puberty.
- Developmentally tonsils arise from the ventral portion of the second pharyngeal pouch, i.e. ideally named as sinus tonsillaris.
- Histologically they consist of lymphoid tissue with aggregates of lymphocytes arranged in follicular manner and embedded in a stroma of connective tissue.
- The tonsil has two surfaces – medial and lateral, and two poles – upper and lower.
Tonsillar crypts
- The medial surface of tonsil has 10-15numbers of pits, which leads into blind ending, and are often highly branched, extending through whole thickness of tonsil – called crypts. Embryologically, they represent sinus tonsillaris.
- The largest crypt is called Crypta Magna / Intra-tonsillar cleft – represent the persistent part of the ventral portion of the second pharyngeal pouch.
- Secondary crypts: They arise from the main crypts within the substance of tonsil.
- Content of crypts: Crypts may be filled with microorganism, desquamated food debris etc. Sometimes they may get impacted in these crypts leading to development of a white material (tonsillolith / tonsil stones) – which can be expressed out with pressure over the anterior tonsillar pillar. This can also lead to acute and recurring inflammation of tonsils (tonsillitis).
Plica triangularis
- Plica triangularis is a semilunar fold of mucous membrane passes from the upper aspect of the palatopharyngeal arch towards the upper pole of tonsil, separating it from the base of the uvula. This creates a potential space called supratonsillar fossa.
- In childhood, plica triangularis is usually invaded by lymphoid tissue and becomes incorporated into the tonsil.
Structures of tonsillar bed from medial to lateral.
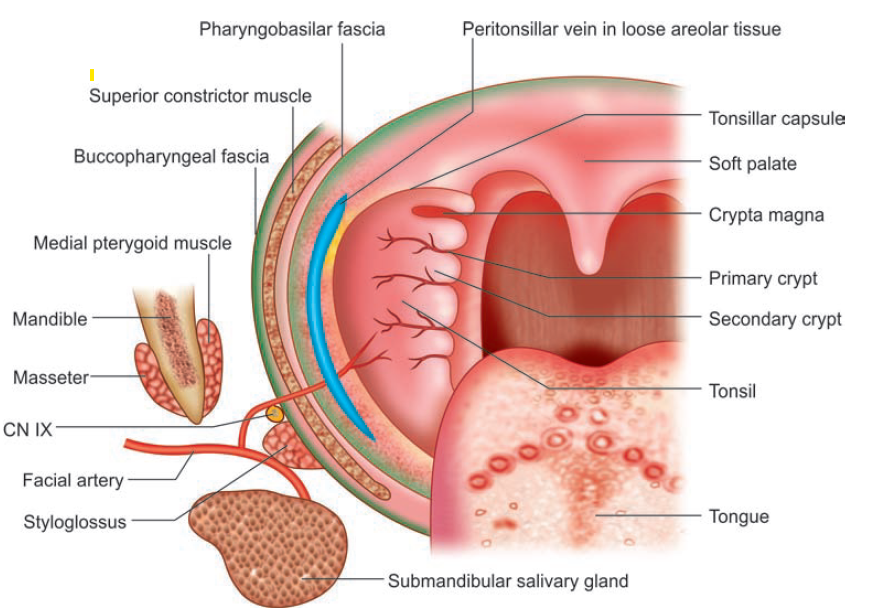
- Condensed capsule formed by the pharyngobasilar fascia and loose areolar tissue – The tonsil is virtually inseparable from its capsule, but the capsule is united by loose connective tissue to superior constrictor muscle. Hence in tonsillectomy the tonsillar dissection is carried out in this plane.
- Just under the capsule is the peritonsillar vein.
- The superior constrictor muscles.
- Buccopharyngeal fascia.
- The glossopharyngeal nerve and the stylohoid ligament pass downwards and forwards beneath the lower edge of the superior constrictor in the lower part of the tonsillar fossa.
Blood supply, Venous drainage and Nerve supply of tonsil
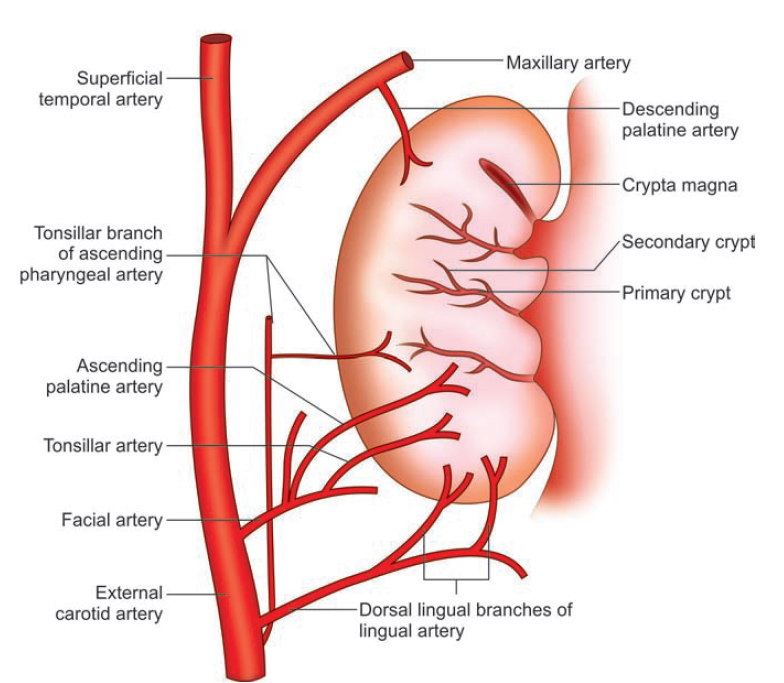
- Tonsillar branch of the facial artery is the main artery of the tonsil.
- It enters tonsil near its lower pole by piercing the superior constrictor just above the styloglossus muscle.
- Lingual artery through its dorsal lingual branches,
- Ascending palatine branch of facial artery,
- Descending palatine branch of maxillary artery
- Ascending pharyngeal vessels.
Venous drainage occurs through the para tonsillar vein (external palatine), and the vessels also pass through to the pharyngeal plexus or facial vein after piercing the superior constrictor to IJV.
The tonsils have no afferent lymphatics. Lymphatic vessels from the tonsil pierce through the buccopharyngeal fascia and pass to the upper deep cervical group of nodes, particularly to the jugulodigastric group.
The sensory nerve supply to tonsil is by:
- Lesser palatine branches from sphenopalatine ganglion of maxillary division of trigeminal nerve (CN V2).
- Glossopharyngeal nerve (CN IX).
Functions of tonsil
- Tonsils are concerned primarily with immunity from pathogens in the ingested food. Germinal centers in these lymphoid organs are located immediately submucosally containing both B and T lymphocytes. B cells are predominant which secretes IgG and IgA
- Contact with allergens in upper respiratory tract therefore enhances local immunity and also contributes to development of systemic immunity.
- Recurrent tonsillitis suggests that there may be some intrinsic defect either in tonsil themselves or in patients immunity.
- IgA production in tonsillar B cells is markedly reduced in children with recurrent tonsillitis.
- There is no evidence that tonsillectomy per se results in impaired immunity, indeed, the converse appears more likely because of extensive backup in immune system.
Common diseases
- Tonsillitis (inflammation of the tonsils) is a clinical condition usually caused by a viral or bacterial infection. The condition is common in children but can occur at any age.
- Most common infection is by Group A beta hemolytic streptococci (GABHS)
- 40% of asymptomatic individuals will also have a culture positivity.
- Other organisms include Hemophilus, Staph. Aureus, Alpha hemolytic strep, Branhamella , Mycoplasma, Chlamyda, anaerobes and respiratory virus.
- This can be acute (recent onset) or chronic (persistent)
- In chornic tonsillitis predominant organism is H.Influenza and S.aureus.
- Other common disease conditions of tonsils are
- Peritonsillitis
- Peritonsillar abscess (quincy)
- Tonsilloliths (tonsil stones): Tonsil stones, or tonsilloliths, are formed when trapped debris within the crypts get hardens or calcifies.
- Common site of impaction of sharp foreign bodies like fishbone.
- Enlarged tonsils in kids and adults can cause obstruction to respiratory airflow and lead to obstructive sleep apnea.
- Malignancies of tonsils
- The tonsillolingual sulcus, which separates the tonsil from tongue, is a common site for carcinoma.
Grading of tonsils
Based on the size of tonsils, following grading system is used to classify them.
| Brodsky grading scale/ AAOHNS Gradation of Tonsillar Enlargement | |||
| Grade | Definition | Description | |
| 0 | Not visible | Tonsils don’t reach tonsillar pillars / Surgically removed. | |
| 1+ | Less than 25% | Tonsils fill less than 25% of transverse oropharyngeal space measured between anterior pillars | |
| 2+ | 25% to 49% | Tonsils fills less than 50% of transverse oropharyngeal space | |
| 3+ | 50% to 74% | Tonsils fills less than 75% of transverse oropharyngeal space | |
| 4+ | 75% or more | Tonsils fills more than 75% of transverse oropharyngeal space | |
| Friedman Grades of tonsillar hypertrophy | |
| Grade 0 | No tonsils seen / Surgically removed tonsils. |
| Grade 1 | Within tonsillar fossa |
| Grade 2 | Visible beyond anterior pillars |
| Grade 3 | Extend 3/4th of way to midline. |
| Grade 4 | Completely obstructing airway i.e. Kissing tonsil. |