Thyroid nodules are a common clinical finding, often detected during routine physical examination or incidentally on imaging. These nodules can be classified as hot (hyperfunctioning) or cold (non-functioning) based on their ability to uptake radioactive iodine or technetium during a nuclear medicine scan. Understanding their functional status is essential for appropriate management and risk stratification.
What Are Hot and Cold Nodules?
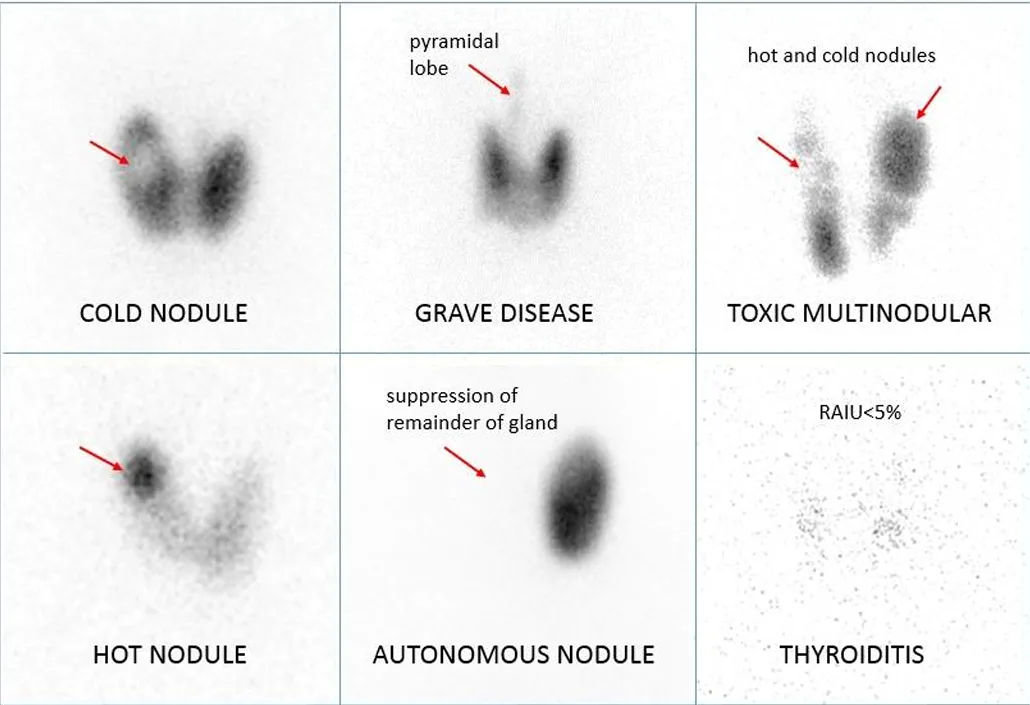
Hot Nodules (Hyperfunctioning Nodules)
Hot nodules are autonomously functioning thyroid nodules that produce thyroid hormones independently of thyroid-stimulating hormone (TSH) regulation. They are typically benign and rarely harbor malignancy.
Characteristics:
- Increased uptake of radioactive iodine (I-131) or technetium (Tc-99m) on a thyroid scan.
- Suppression of TSH due to excessive hormone production.
- Often present as a single nodule (toxic adenoma) or multiple nodules (toxic multinodular goiter, TMNG).
- Associated with thyrotoxicosis, presenting symptoms like weight loss, palpitations, and heat intolerance.
Cold Nodules (Non-Functioning Nodules)
Cold nodules are non-functioning thyroid nodules that do not produce thyroid hormones and appear as areas of reduced or absent uptake on a thyroid scan. These nodules have a higher likelihood of malignancy compared to hot nodules.
Characteristics:
- No uptake of radioactive iodine or technetium.
- Can be benign (most cases) or malignant (requiring further evaluation).
- No suppression of TSH levels; TSH remains normal or elevated.
- May be solid, cystic, or complex in structure.
- Require further assessment using ultrasound and fine-needle aspiration (FNA) biopsy if suspicious.
Diagnosing Hot vs. Cold Nodules
A. Clinical and Biochemical Markers
- Serum TSH Levels:
- Low TSH: Suggests a hyperfunctioning nodule (hot nodule).
- Normal/High TSH: Suggests a non-functioning nodule (cold nodule), requiring further imaging.
B. Imaging Modalities
- Technetium (Tc-99m) or Radioactive Iodine (I-131) Uptake Scan
- Hot nodules show increased uptake.
- Cold nodules show reduced or absent uptake.
- Ultrasound (Preferred for Cold Nodules)
- Helps assess size, echogenicity, vascularity, and suspicious features (e.g., irregular margins, microcalcifications, taller-than-wide shape).
- Fine-Needle Aspiration (FNA) Biopsy
- Recommended for cold nodules with suspicious ultrasound features to rule out malignancy.
Clinical Implications and Management
Hot Nodules
- Asymptomatic: Can be monitored.
- Symptomatic (Thyrotoxicosis): Treated with:
- Radioactive iodine (RAI) therapy to ablate the nodule.
- Surgical excision if large, causing compression, or RAI is contraindicated.
- Antithyroid medications (temporary) to control symptoms preoperatively.
Cold Nodules
- Benign on FNA: Regular follow-up with ultrasound.
- Suspicious or Malignant Features: Surgical intervention (lobectomy or total thyroidectomy) depending on risk factors and histopathology.
Key Takeaways
- TSH levels guide initial suspicion: Low TSH suggests a hot nodule, while normal/high TSH suggests a cold nodule.
- Tc-99m/I-131 scans are useful for thyrotoxicosis but not routinely recommended for cold nodules.
- Ultrasound and FNA are preferred for cold nodules, as they help determine malignancy risk.
- Hot nodules are rarely malignant, whereas cold nodules require thorough evaluation for potential malignancy.
Conclusion
The distinction between hot and cold nodules is crucial for clinical decision-making. While hot nodules are often benign and managed based on symptoms, cold nodules warrant careful assessment with ultrasound and biopsy to rule out malignancy. A strategic approach involving biochemical, imaging, and cytological evaluation ensures optimal patient care and outcomes.