Malignancies arising in nasopharynx / nasopharyngeal carcinoma (NPC) have different natural behavior and therapeutic consideration than other head and neck cancers.
Nasopharyngeal carcinoma also has a very skewed geographic and ethnic distribution, with 80% of the global burden in Asian countries.
What’s new in staging of nasopharyngeal carcinoma?
The TNM staging system developed by the International Union against Cancer (UICC) and American Joint Committee on Cancer (AJCC) is considered the authoritative system for assessing disease progression, predicting prognosis and assisting treatment selection. Currently, AJCC Version 8 is used for the staging of nasopharyngeal carcinoma.
Development of accurate imaging modalities, advances in radiotherapy techniques like intensity-modulated radiotherapy (IMRT), use of combination chemotherapy has improved the management and survival outcome of NPC in the past two decades. Hence a different staging and prognostic system are developed for nasopharyngeal carcinoma.
This article focuses on TNM staging for epithelial tumors of the nasopharynx and the changes in version 8 of the AJCC system. The staging system for nonepithelial tumors such as mucosal melanoma, lymphoma, and sarcoma of soft tissue, bone, and cartilage are not included in this article.
T Staging
In TNM staging of cancer, T describes the size of the original (primary) tumor and whether it has invaded nearby tissue.
The following are major changes in the definition of primary tumor (T) staging of nasopharyngeal carcinoma in AJCC 8.
- T0 is added for Epstein-Barr virus (EBV) positive unknown primary with cervical lymph node involvement. The prognostic stage group is defined in the same way as TI (or Tx).
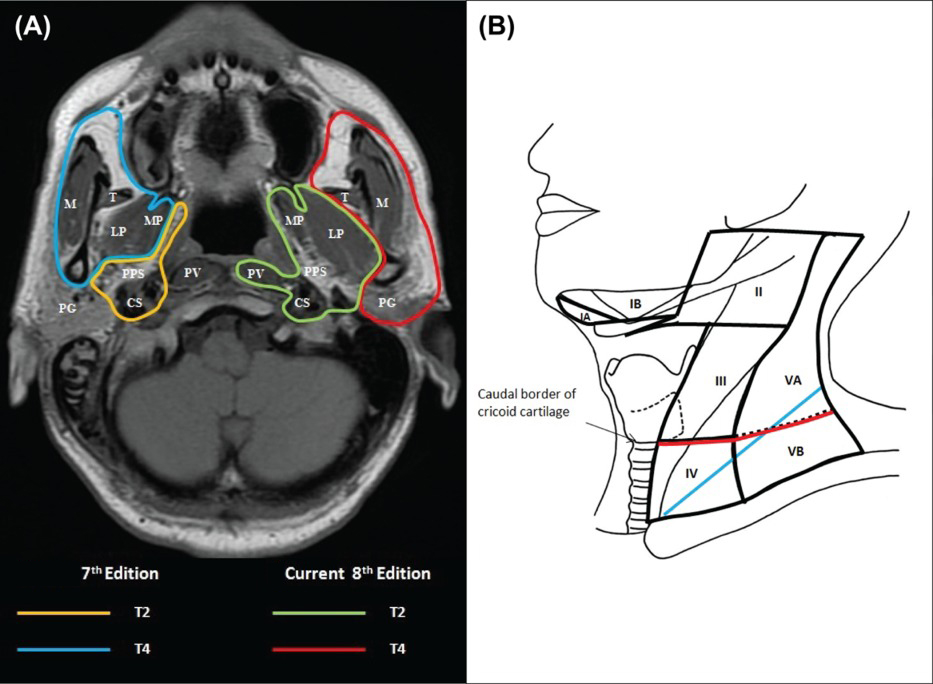
- The ambiguous definition of infratemporal fossa (ITF)/masticatory space (MS), which was regarded as T4 in the 7th edition, has been replaced by a more specific description in the 8th edition.
- In the AJCC Cancer Staging Manual seventh edition, the involvement of any masticator space structure was designated T4 disease. This has now been subdivided so that involvement of the medial or lateral pterygoid muscle or of the prevertebral muscles is T2 disease, but if there is an extension of tumor beyond the lateral surface of the lateral pterygoid muscle or involvement of the parotid gland, this is T4 disease.
- Adjacent muscle involvement (including medial pterygoid, lateral pterygoid, and prevertebral muscles) is now down staged to T2.
- The involvement of any bony structures such as cervical vertebrae, pterygoid plates, skull base, or paranasal sinuses is T3 disease.
| 7th edition | 8th edition | |
| T0 | No tumor identified, but EBV-positive cervical node involvement. | |
| T1 | Nasopharynx, oropharynx or nasal cavity | Nasopharynx, oropharynx, nasal cavity without parapharyngeal involvement |
| T2 | Parapharyngeal extension | Parapharyngeal space and/or adjacent soft tissue involvement (medial pterygoid, lateral pterygoid, prevertebral muscles) |
| T3 | Bony structures and/or paranasal sinuses | Bony structures at the skull base, cervical vertebra, pterygoid structures, and/or paranasal sinuses |
| T4 | Intracranial extension and/or cranial nerves, hypopharynx, orbit or infratemporal fossa/masticatory space. | Intracranial extension, the involvement of cranial nerves, hypopharynx, orbit, parotid gland and/or extensive soft tissue infiltration beyond the lateral surface of lateral pterygoid |
N Staging
Distribution and prognostic impact of regional lymph node spread from nasopharynx cancer, particularly of the undifferentiated type, are different from those of other head and neck mucosal cancers and justify the use of a different N classification scheme.
Nasopharyngeal carcinoma often presents with early lymphatic spread. The retropharyngeal nodes and the cervical nodes (both jugular and spinal accessory chains) are involved, often bilaterally. The lymphatic spread in NPC follows a predictable and orderly pattern from upper to lower neck.
“skip” metastasis is rare.
Following are changes in the N category classification,
- Replacement of supraclavicular fossa with anatomical lymph node levels: In the seventh edition staging system, N3a indicates any nodal mass measuring 6 cm that lies above the supraclavicular fossa and N3b disease was determined by the presence of 1 supraclavicular node in the triangle of Ho (subclavian triangle or supraclavicular triangle, omoclavicular triangle).
In the 8th edition, N3a and N3b in the 7th edition were merged into a single N3 category, which is now defined as unilateral or bilateral metastasis in cervical lymph node(s), larger than 6 cm in greatest dimension, and/or extend below the caudal border of the cricoid cartilage.
| 7th edition | 8th edition | |
| N0 | None | None |
| N1 | Unilateral cervical and/or unilateral or bilateral retropharyngeal node(s), ≤ 6 cm in greatest dimension, above supraclavicular fossa | Unilateral cervical and/or unilateral or bilateral retropharyngeal node(s), ≤ 6 cm in greatest dimension, above the caudal border of the cricoid cartilage |
| N2 | Bilateral cervical node(s), ≤ 6 cm in greatest dimension, above supraclavicular fossa | Bilateral cervical node(s), ≤ 6 cm in greatest dimension, above the caudal border of the cricoid cartilage |
| N3 | N3a > 6 cm in greatest dimension, above supraclavicular fossa | Unilateral or bilateral cervical node(s), > 6 cm in greatest dimension, below the caudal border of the cricoid cartilage |
| N3b in the supraclavicular fossa |
In clinical evaluation, the maximum dimension (in any direction) of the nodal mass, the laterality, and the lowest level of neck involvement should be assessed.
Midline nodes are considered ipsilateral nodes. Nodal size larger than 6 cm in greatest dimension and/or extension below the caudal border of the cricoid cartilage is associated with the worst prognosis.
The involvement of lymph nodes below the clavicle (including mediastinum, infraclavicular region, axilla, or groin) is considered as distant metastases.
M Staging
In TNM Classification of tumors, M Staging denotes distant metastasis. That is the spread of the tumor to another faraway location.
Nasopharyngeal carcinoma is notorious for a high risk of distant metastasis. The most common sites include lung, bone, liver, and distant lymph nodes. As mentioned earlier in the N classification, the involvement of lymph nodes below the clavicle (including mediastinum, infraclavicular region, axilla, or groin) is considered as distant metastases.
| M0 | No distant metastasis |
| M1 | Distant metastasis present |
Role of Pathological Staging
Unlike other head and neck cancer, the primary treatment of nasopharyngeal carcinoma is by radiotherapy, with or without chemotherapy, with no resection of primary cancer. This makes pathological classification largely irrelevant. Surgery to primary or neck nodes is considered in nasopharyngeal carcinoma only for recurrence.
Prognostic staging
Based on the overall T, N and M staging, prognostic staging has been done.
The following are the changes in prognostic staging system for nasopharyngeal carcinoma.
- Stages IVA (T4) and IVB (N3) of the 7th edition were merged into stage IVA.
- The previous stage IVC was upgraded to stage IVB in the new edition.
| Stage 0 | Tis | N0 | M0 |
| Stage I | T1 | N0 | M0 |
| Stage II | T1, T0 | N1 | M0 |
| T2 | N0, N1 | M0 | |
| Stage III | T0, T1, T2, T3 | N2 | M0 |
| T3 | N0, N1, N2 | M0 | |
| Stage IVA | T4 | Any N | M0 |
| Any T | N3 | M0 | |
| Stage IVB | Any T | Any N | M1 |
References
- Gospodarowicz MK, Brierley JD, Wittekind C, editors. TNM classification of malignant tumours. John Wiley & Sons; 2017 Jan 17.
- 8th Edition of the UICC TNM classification of Malignant Tumors published.
- J.J. Pan, W.T. Ng, J.F. Zong, et al. Proposal for the 8th edition of the AJCC/UICC staging system for nasopharyngeal cancer in the era of intensity-modulated radiotherapy Cancer, 122 (4) (2016), pp. 546-558