Otitis Media with Effusion (OME) is a clinical condition of ear characterized by chronic accumulation of serous / mucoid fluid within the middle ear or mastoid air cells for more than 12 weeks duration.
Also known as glue ear, Serous otitis media, Secretory otitis media, Chronic non purulent otitis media
Pathology
- The ciliated, pseudostratified columnar epithelium of respiratory tracts extends into anterior part of middle ear and hypotympanum via eustachian tube. In addition, there are Goblet cells and mucus secreting glands.
- When middle ear inflammation occurs, the normal, flat cuboidal middle ear and mastoid mucosa is patchily replaced by thickened pseudostratified mucus epithelium with varying degrees of specialization, such as development of cilia. In addition, there will be proliferation of goblet cells and mucus secreting glands.
- Submucosa becomes edematous, inflamed with macrophage, plasma cells and lymphocytes infiltration.
- This will cause exudation of inflammatory fluids.
- The fluid will be made of a mixture of secretions of the epithelial cells, the goblet cells and the mucus glands along with inflammatory transudates / exudates.
- It is the mucin in the secretions which is responsible for variable viscosity of middle ear fluids.
- The ciliary lining is less efficient to move these thick secretions into nasopharynx than normal.
- These secretions when get secondarily infected with bacteria causes acute otitis media.
- Once infection is resolved, it will take some time for epithelium to recover. So OME will be present temporarily in many children after an episode of acute otitis media.
Etiology
- Infections
- In adults, sinusitis is considered as main correlating disease.
- Streptococcus pneumoniae > H. Influenza > Moraxella
- In children, even in long standing cases rarely only pathogens identified.
- Viral upper respiratory tract infection is the most common cause.
- The incidence of pathogens was higher in younger children (less than 2 years) and in those with recurrent upper respiratory tract infection and recurrent acute otitis media.
- When isolated streptococcus pneumonia was the most commonly isolated one.
- In adults, sinusitis is considered as main correlating disease.
- Acute otitis media (AOM) in children
- This is likely to be the largest single factor for developing OME.
- Each episode of AOM increases odds ratio for OME by 12
- No evidence that management of AOM with antibiotics makes any difference in chance of having an OME later.
- Role of Biofilms in OME
- Are a matrix of polysaccharides formed by colonies of bacteria that protect them by forming a favorable environment.
- Shields them from eradication by host tissue and antibiotic therapy.
- Cause release of inflammatory cytokines TNFa, IL1b etc.
- Activation of arachidonic acid metabolism, histamine, platelet activating factor, adhesion cell molecules.
- Leads to differentiation of basal cells of mucosa to goblet cells to form submucous glands.
- Secretion of mucin by cells as a method of immune clearance.
- Allergy
- Radio allergent Sorbant Assay (RAST), Patch test, Serum IgE levels, Eosinophils cation protein etc. shows allergy as an etiology.
- Nasopharyngeal pathologies
- Nasopharyngeal lymphoid hypertrophy
- Secondary to chronic nasopharyngeal infection in adenoid tissue.
- Branchial cysts
- Nasopharyngeal carcinoma
- Eustachian tube cartilage erosion
- Obstruction of the inlet
- Tensor veli palatine invasion / destruction
- Wegener’s granulomatosis.
- Exposure of ears, nasopharynx, eustachian tube to radiation (e.g. treatment of nasopharyngeal carcinoma).
- Functional eustachian tube obstruction
- Edema / blockage /Atrophy of nasopharyngeal orifice
- Inflammation of tube due to allergy, LPR, GERD, pollutants such as cigarette smoke, biofilm, cleft palate.
- GERD – Pepsin is present in high amount (80%) of effusions.
- Craniofacial abnormality like cleft palate – deficient palatine muscles and resultant poor tube function. The disease is extremely persistent. Children with Down / Turner syndrome also found to have high incidence of OME while those with bifid uvula have no increased risk.
- Eustachian tube can be obstructed during barotrauma and hyperbaric O2 therapy.
- Mastoid pneumatization
- Poor mastoid pneumatization is also a risk factor.
- Hereditability
- There was a greater concordance among monozygotic sets in number, duration of OME than in dizygotic.
- Race
- Black = White.
- Chinese children have less prevalence.
- Gender
- No difference among boys and girls.
- If any, Boys > Girls
- Miscellaneous
- Surgery of head and neck
- Prolonged intubation
- Multiple myeloma
- Cystic fibrosis
- Immune deficiency syndrome.
- Prevention of otitis media with effusion
- Breast feeding – Numerous studies indicate that breast-feeding can decrease this risk by transmitting antibodies from mother to child and reducing environmental allergies.
- Removing tobacco smoke from the child’s environment.
- Good hand hygiene and pneumococcal vaccination may reduce the development of AOM.
- Limiting pacifier use in children <18 months old decreases the incidence of AOM by about 30%.
Prevalence of otitis media with effusion
- Lower incidence in adults than in children.
- In kids,
- common problem affecting 60% of children before 2 years of age.
- about 90% of children have OME before school age and they develop, on average, 4 episodes of OME every year.
- the disease prevalence is usually bimodal with
- First and largest peak at 2 years – when they attend play school.
- Second peak at 5 years – when they attend primary school.
- Winter: Summer = 2:1
- This may be due to increased frequency of upper respiratory tract infection and ear infections in winter.
- Greater chance of passing them on between children because of closer contact in cold weather.
- Laterality
- Unilateral OME is twice more common than bilateral OME.
Clinical presentation
- Hearing loss, ear fullness, clogged ear sensation, pulsatile / crackling tinnitus.
- Autophony
- In many children OME is preceded with otalgia and fever due to associated AOM.
- Unresolved OME and associated hearing loss may lead to language delay, auditory problems, poor school performance, and behavioral problems in young children.
Diagnosis of otitis media with effusion
- Diagnosis of OME is clinical and can be confirmed by tympanometry.
- History
- If an infant’s parents give history of ear problems, recurrent URTI, mouth breathing and snoring such a child is more likely to have OME.
- Diagnostic tools
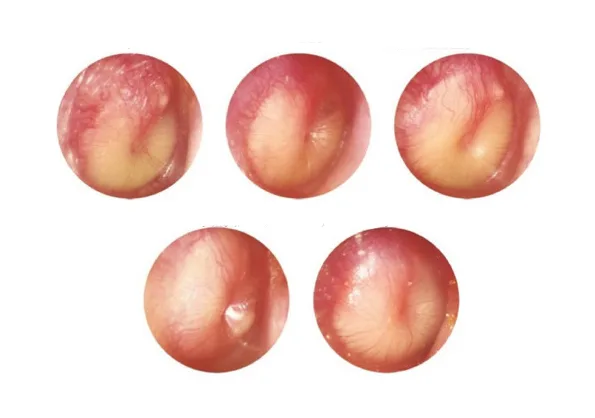
- Otoscopy
- Otoscopy should be done in all children.
- Different combinations of retractions of pars tensa of tympanic membrane, neo-annular fold formation, and variations in color (more yellow, amber, more blue or just clear).
- Scarring of tympanic membrane, Myringosclerosis
- Fluid levels or amber colored effusion with air bubbles.
- Pneumatic otoscopy
- Pneumatic otoscopy is of added value.
- This is recommended as the primary diagnostic method – immobility on pneumatic otoscopy is diagnostic
- If the tympanic membrane is moving middle ear is aerated.
- The sensitivity ranges from 85 to 93% and specificity from 71 to 89%
- Video otoscopy
- Can be documented and used to monitor changes.
- Can be used for teaching and research purposes.
- Otoscopy
- Audiometry
- In those with OME on otoscopy, and with suspected hearing impairment audiometry is mandatory.
- Conventional air-bone conduction testing is the preferred method – separately measures each ear and can quantify any conductive component present.
- AB gap
- The presence of AB gap of at least 10dB is a poor predictor of concurrent OME – chance of a dry tap (getting fluid during tympanotomy) is 37%.
- Only when the AB gap is more than 30dB the chance of dry tap reduces to less than 4%.
- OME, on average, produces a 10- to 15-dB decrease in hearing levels, which results in an average hearing loss of 28 dB, while a lesser proportion (approximately 20%) exceed 35-dB hearing loss.
- Carhart’s notches
- Reported to be present in 48% of children.
- Positive predictive value of Carhart notch in diagnosing fluid at myringotomy was 97%.
- Tympanometry
- Tympanometry with an impedance meter – Is confirmatory and considered as reference standard.
- Type B / C1 / C2 tympanogram along with an air bone gap of more than or equal to 10dB highly suggestive of OME
- Absent reflexes
- Otoscopy suggests OME + Type B curve = 98% sensitive
- Otoscopy suggests no OME + Type A curve = 98% specificity
- Tympanoscopes
- Tympanometry can also be performed with a handheld otoscope which automatically prints out the results.
- Advantage of portability and low cost.
- Acoustic reflexes
- Not advocated
- Performed with a handheld acoustic otoscope which doesn’t require a seal. It is moved around while emiting a sound of 80dB over a frequency range. The amount of sound reflected back is recorded and analyzed in various ways – But the sensitivity and specificity of this test is poor than tympanometry.
- ET function tests
- Sonotubometry – Needs further improvement.
- Imaging
- Rarely needed.
- Gold standard – MRI
- CT / MRI shows opacification of ME and mastoid air cells without erosion of mastoid septa.
- Surgery
- In children who are being operated for OME, surgical finding is considered as reference standard.
- Myringotomy or tympanocentesis
- Absence of fluid in middle ear doesn’t rule out OME as fluid can present in mastoid but not in mesotymapanum.
- In children who are being operated for OME, surgical finding is considered as reference standard.
- Fluid cytology
- Children – More mucus
- Adult – More serous
- Effusion lacks inflammatory cells but contains bacterial colonies.
- Screening of children for OME
- Not recommended for children who are not “at risk” (explained later) and do not have symptoms that may be attributable to OME, such as hearing difficulties, balance (vestibular) problems, poor school performance, behavioral problems, or ear discomfort.
- Assessing for OME at 12 to 18 months of age is recommended in “at risk” children because this is an especially critical period for language, speech, balance, and coordination development.
Differential diagnosis
- Traumatic CSF leak
- Myringotomy in such conditions can cause persistent CSF leakage / leading to meningitis.
Treatment of otitis media with effusion
- Wait and watch policy.
- In general, OME is a benign condition with a high spontaneous recovery rate and no long-term sequel.
- It should be explained to parents that impairment associated with OME is very variable in degree and mild or moderate at most.
- Clinicians should manage the child with OME who is not “at risk” (see later) with watchful waiting for 3 months from the date of effusion onset (if known) or 3 months from the date of diagnosis (if onset is unknown).
- If OME is asymptomatic and is likely to resolve spontaneously, intervention is usually unnecessary, even if otitis media with effusion persists for >3 months.
- Risk factors associated with reduced likelihood of spontaneous resolutions.
- longer duration
- bilateral OME
- onset of OME in summer or fall season,
- hearing loss 30-dB HL in the better-hearing ear,
- history of prior tympanostomy tubes, and
- not having a prior adenoidectomy
- Clinicians should reevaluate, at 3- to 6-month intervals, children with chronic OME until the effusion is no longer present, significant hearing loss is identified, or structural abnormalities of the eardrum or middle ear are suspected.
- The mean overall duration for spontaneous recovery is 1.8 months with 12% lasting more than 6 months.
- Counselling and Hearing tactics
- In most children, main concern is hearing.
- Disability can be minimized by hearing tactics.
- getting the child’s attention before starting to talk;
- facing the child so that they can see you talk;
- reducing the background noise as much as possible by turning off the television, etc;
- speaking in a normal voice both in volume, speed and emphasis, as close as possible to the child;
- Use short, simple sentences and comment on what the child is doing;
- When speaking to the child, slow down, raise the sound level, and enunciate clearly;
- Read to or with the child, explaining pictures and asking questions;
- Call attention to the sounds and spelling of words when reading;
- Patiently repeat words, phrases, and questions when misunderstood;
- In the classroom, ensure that the child sits near the teacher in the front of the room;
- If further assistance in the classroom is necessary, use a remote microphone personal or sound field amplification system.
- Rule out Nasopharyngeal carcinoma
- Especially in adults with OME, Neck nodes
- Posterior rhinoscopy
- Rigid Hopkins / Flexible endoscopy is recommended.
- Biopsy of suspicious lesions
- Screening blood test for EBV – IgA-VCA, IgA-EA, EB-DNA
- Auto inflation
- By performing Valsalva
- Less value in chronic cases.
- Children allocated to auto inflation were 3.5 times more likely to improve than control. If some form of non-surgical management is required during a watchful waiting period, auto inflation therapy has strongest evidence.
- Medical
- Oral or Intra nasal corticosteroids
- Insufficient evidence to support use of topical nasal steroids for OME.
- At present, guidelines (2016 AAOHNS) don’t recommend usage of steroids.
- Antibiotics
- Guidelines don’t recommend usage of antibiotics. (2016 AAOHNS) except when associated illnesses are present that would benefit from antibiotics, such as acute bacterial sinusitis or group A streptococcal infection.
- Antihistamine / Nasal decongestants
- Antihistamine / decongestants had no significant effect on resolution rate of OME.
- Clinicians should recommend against using antihistamines, decongestants, or both for treating OME. (2016 AAOHNS)
- Decrease surface tension.
- Ambroxol, Acetyl cysteine – 30mg TDS for 15 days
- If viral etiology, start early antivirals.
- Oral or Intra nasal corticosteroids
- Surgical
- Not shown to be effective in restoring hearing levels.
- Myringotomy and aspiration
- Hearing impairment is not relieved but continues to recur.
- Myringotomy and ventilation tube insertion.
- Can be categorized as Grommets or T Tubes.
- Should be offered to children aged >=6 months with documented bilateral OME for >3 months and documented hearing difficulties.
- For children who do not receive tympanostomy tubes, a follow-up schedule to monitor OME and hearing levels should be determined based on the specific needs of the child. This may be more frequent than routine 3- to 6-month intervals. Children should be monitored until OME resolves in all affected ears.
- Surgical treatment of causative factor like adenoids (2016 AAOHNS Guidelines)
- For child < 4 years old, adenoidectomy should not be performed unless a distinct indication (e.g., nasal obstruction, chronic adenoiditis) exists other than OME.
- For child 4 years or older,
- Tympanostomy tube placement alone, which offers the most reliable short- and intermediate-term resolution of hearing loss associated with OME, but has minor complications associated with tube.
- Adenoidectomy alone, which offers comparable rates of OME control compared with tympanostomy tubes at 6 and 12 months,205 but may have a less reliable impact in the short term. May need additional surgery for tympanostomy tube insertion later.
- Adenoidectomy plus myringotomy (without tubes), which includes aspiration of effusion and possible lavage of the middle ear space with saline solution, has outcomes comparable to tubes with less otorrhea and tympanic membrane.
- Adenoidectomy plus tympanostomy tube placement, which offers the combined benefits of both procedures, especially the ability to reduce repeat surgery in children with a history of tympanostomy tube placement.
| Evidence-Based Recommendations for Tympanostomy Tube Insertion. | ||
| Statement | Action | Strength |
|---|---|---|
| Chronic bilateral otitis media with effusion (OME) with hearing difficulty | Clinicians should offer bilateral tympanostomy tube insertion to children with bilateral OME for ≥3 mo (chronic OME) AND documented hearing difficulties. | Recommendation |
| Chronic OME with symptoms | Clinicians may perform tympanostomy tube insertion in children with unilateral or bilateral OME for ≥3 mo (chronic OME) AND symptoms that are likely attributable to OME that include, but are not limited to, vestibular problems, poor school performance, behavioral problems, ear discomfort, or reduced quality of life. | Option |
| Recurrent acute otitis media (AOM) with middle ear effusion (or OME) | Clinicians should offer bilateral tympanostomy tube insertion to children with recurrent AOM who have unilateral or bilateral middle ear effusion (or OME) at the time of assessment for tube candidacy. | Recommendation |
| Tympanostomy tubes in at-risk children | Clinicians may perform tympanostomy tube insertion in at-risk children with unilateral or bilateral OME that is unlikely to resolve quickly as reflected by a type B (flat) tympanogram or persistence of effusion for ≥3 mo (chronic OME). | Option |
| Recommendations for NOT performing tympanostomy tube insertion | ||
| OME of short duration | Clinicians should NOT perform tympanostomy tube insertion in children with a single episode of OME of <3 month of duration. | Recommendation (against tubes) |
| Recurrent AOM without middle ear effusion (or OME) | Clinicians should NOT perform tympanostomy tube insertion in children with recurrent AOM who do not have middle ear effusion (or OME) in either ear at the time of assessment for tube candidacy. | Recommendation (against tubes) |
| From the American Academy of Otolaryngology—Head and Neck Surgery Foundation’s clinical practice guideline on tympanostomy tubes; refer to the guideline for details on the evidence and rationale underlying each recommendation. | ||
- Hearing aids
- Main management option
- Improvement is in range as expected of ventilation tubes.
- Main concern is noise trauma once OME is resolved.
- BAHA
- No chance of noise trauma.
- Other treatment options
- Mastoidecomy
- Percutaneous mastoid ventilation etc.
Outcomes of childhood OME
- About 75% of children with OME resolve by 3 months when it follows an episode of AOM.
- Children under three years of age have a propensity for bilateral OME, the effusion lasted on average ten weeks, and they were likely to have further episode within weeks.
- Older children between 3-7 years – watchful waiting for 9 months – 92% of OME associated hearing problem resolves (spontaneous resolving)
- 14% can go into attic retractions.
- Tympanosclerosis and atrophy of pars tensa are OME disease effects, the risk of which is increased by insertion of ventilation tubes to >45% and around 70% respectively.
- Long term pars tensa retractions are more likely to cause by insertion of ventilation tube.
- Most of the children with Bilateral OME have an insufficient hearing impairment to be materially disabling.
- They may have a residual hearing impairment in order of 10dB – likely due to ossicular chain immobility caused by some residual fluid or mucosal oedema around them.
- SNHL – No evidence to suggest that OME is associated with SNHL in short term.
- Speech and language development – A mild effect on speech production and reception in early childhood which is not modified by surgical intervention and spontaneous resolving with age.
- Behavior – Some evidence that when child reach age of 15, they have still poorer behavior than non OME children.
- Balance – Insufficient knowledge and understanding to guide the assessment and management of balance symptoms in OME.
- Quality of life – Has been shown to improve in children with ventilation tube insertion.
At risk kids
- Permanent hearing loss independent of otitis media with effusion
- Suspected or confirmed speech and language delay or disorder.
- Autism spectrum disorder and other pervasive developmental disorders
- Syndromes (e.g., Down) or craniofacial disorders that include cognitive, speech, or language delays.
- Blindness or uncorrectable visual impairment
- Cleft palate, with or without associated syndrome
- Developmental delay
Patient Resources
References
- Clinical Practice Guideline: Otitis Media with Effusion (Update) – Richard M. Rosenfeld, Jennifer J. Shin, Seth R. Schwartz, Robyn Coggins, Lisa Gagnon, Jesse M. Hackell, David Hoelting, Lisa L. Hunter, Ann W. Kummer, Spencer C. Payne, Dennis S. Poe, Maria Veling, Peter M. Vila, Sandra A. Walsh, Maureen D. Corrigan, 2016 (sagepub.com)
- England, R.J., & Shamil, E. (Eds.). (2021). Scott-Brown’s Essential Otorhinolaryngology, Head & Neck Surgery (1st ed.). CRC Press. https://doi.org/10.1201/9781003175995