Mammary analog secretory carcinoma (MASC), also known as secretory carcinoma, is a recently identified type of low-grade malignant tumor found in salivary glands. It has been officially recognized in the 4th edition of the WHO classification of head and neck tumors. MASC is characterized by a specific chromosomal translocation, t(12;15)(q13;q25), which involves the fusion of the ETS variant 6 gene (ETV6) with the neurotrophic tyrosine kinase receptor type 3 (NTRK3) gene. This fusion results in identical histological, immunophenotypic, and molecular features to secretory carcinoma found in the breast.
The discovery of MASC was first reported by Skalova et al. in 2010. Before its identification, MASC was often misdiagnosed as various other types of salivary gland tumors, most commonly zymogen-poor Acinic Cell Carcinoma and Adenocarcinoma, not otherwise specified (NOS). Since its recognition, approximately 90 cases have been documented in the literature. The parotid gland is the most frequently reported site of origin, with the majority of cases being documented through case reports with literature reviews.
Due to its rarity, there is limited information available in the literature regarding the clinical characteristics, optimal treatment strategies, the necessity for additional treatments, prognostic factors, and specific survival rates associated with this neoplasm. The most extensive cohort of MASC patients, consisting of 55 individuals, was recently published.
Case report
A 49-year-old, man with no comorbidities presented to us with complaints of swelling in right parotid region for a period of 6 years, with gradual increase in size for the last 2 months. The swelling was not associated with pain, fever or facial deviation. On examination a hard, non tender swelling measuring 3 × 4cm with lobulated margins was palpable in the retromandibular fossa and adjacent tail of the parotid. Oral cavity and oropharynx were normal. Facial nerve functions were intact and no regional lymph nodes were palpated.
Fine needle aspiration (FNA) from the lesion proved it to be salivary gland carcinoma with high grade areas, suggestive of acinic cell carcinoma. Ultrasonography of the neck showed a well differentiated lobulated hypoechoic lesion in the superficial lobe of right parotid with extension to deep lobe. Magnetic resonance imaging of the neck further revealed a 3.4× 2cm mass in superficial lobe of right parotid extending to deep lobe with a small volume ipsilateral level II lymph node. No obvious nerve thickening or infiltration was seen.
With a provisional diagnosis of parotid carcinoma, after a multidisciplinary tumor board (MDT) meeting, a total conservative parotidectomy with right lateral neck dissection (II-IV) was planned and executed uneventfully. A 4 × 4cm tumor was seen in the superficial lobe of right parotid gland with minimal extension to deep lobe. No significant cervical lymph nodes were harvested.
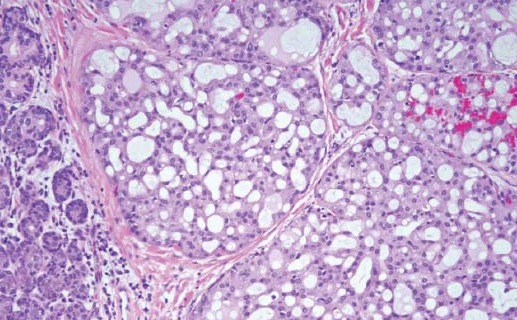
The final histopathology report was that of a 4.5 × 2 × 1.5 cm nodular mass in right superficial lobe of parotid, with cut section of nodule showing grey-white to yellowish and glistening areas which were firm to hard in consistency. There was no tumor necrosis, perineural infiltration or lymphovascular emboli and the resected margins were free of tumor.
Morphology and immunohistochemical features of the lesion were consistent with mammary analogue secretory carcinoma with focal solid areas showing nuclear atypia and occasional mitosis. Immunohistochemistry of the tumor cells were found to be S100 diffuse positive and DOG1 negative. Rest of the tissues was unremarkable and of the 24 nodes identified, none showed metastasis.
A discussion with the pathologists revealed that the final HPR had to be changed because the cells in the final specimen did not appear as aggressive as aspirate in the FNA and hence after a repeat MDT meeting we kept the patient on follow up alone.
Our patient was diagnosed at an early stage, showing no notable signs of neck node involvement through clinical or radiological assessments. Consequently, it was debatable whether an extensive neck dissection was necessary. However, given the limited number of patients included in many of the existing case series, further investigation is required to ascertain whether elective neck dissection should be considered as a standard approach for early-stage MASC cases.