
Incomplete Partition type III (IP-III) or most widely known as X linked deafness is an inner ear anomaly associated with congenital mixed hearing loss, fixation of stapes footplate and perilymph gusher during stapes or cochlear implant surgery.
Phippard addressed this anomaly as pseudo-Mondini stage II and described as partial hypoplasia of the cochlea, stapes fixation, dilated internal auditory canal (IAC) and abnormal communication with the base of the cochlear duct.
Epidemiology
Incomplete cochlear partition constitutes approximately 41% of whole inner ear malformations.
Incomplete Partition-III is the rarest type of inner ear malformation, which constitutes 2% of the cases.
Pathophysiology
The normal otic capsule is a three-layered structure. The inner endosteal layer receives blood supply from the inner ear, while the middle enchondral layer and the outer periosteal layer receives blood supply from the middle ear.
The exact cause of cochlear malformations lies in the genetic mutations in IP-III. Mutation of DFN3 gene in locus 21 of the short arm of chromosome X (Xq21) will lead to deafness with congenital stapes footplate fixation. This mutation will lead to the formation of a thin otic capsule around the cochlea. Because of reduced or absent blood supply from the middle ear, the second (middle enchondral) and third (outer periosteal) layers of otic capsule are either absent or very thin. Hence the otic capsule in case of IP-III will follows the outline of the membranous labyrinth as if it is formed by a thick endosteal layer.
The reduced blood supply will also lead to the defective cochlear base formation. This will cause the failure of modiouls to form attachment points leading to the characteristic radiologic finding of the absent modiolus.
Clinical features
Female heterozygous carriers are having normal hearing or mild hearing loss. Severe-profound mixed hearing loss (MHL) is the characteristic audiological finding in IP-III.
Young males with congenital mixed type hearing loss should be studied with HRCT of the temporal bone to avoid unnecessary stapes surgery.
Reasons for mixed hearing loss in IP-III
Sennarolu et al in their study observed that sensory neural hearing loss (SNHL) is due to modiolar defects while the conductive component (CHL) is due to associated stapedial fixation.
Tang and Pames et al in their study mentioned that, intracranial pressure is transmitted into the perilymphatic space, and the raised perilymphatic pressure that is exerted on the cochlear duct and the stapes footplate results in a mixed pattern of SNHL and CHL respectively.
Snik et al. in their study explained the air-bone gap with the third window phenomenon. They reported that because of the congenital malformation audiovestibular system functioned more effective than normal system leading to better bone conduction levels. They revealed that audiological studies were in accordance with pure SNHL and an air-bone gap in the audiogram did not have the significance of CHL component.
The radiological findings of IP-III type cochlea are as follows.
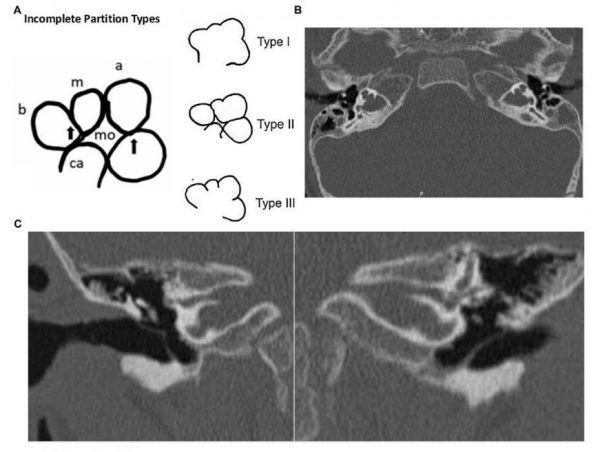
- Complete absence of modiolus
- Partial interscalar septae
- Very thin otic capsule.
- Absence of the septum (lamina cribrosa) between the base of the cochlea and Internal Acoustic Canal (IAC).
- Incomplete separation of the coils of the cochlea from the IAC
- Cochlea will be placed directly at the lateral end of IAC that in its usual anterolateral position.
- External dimensions of the cochlea do not differ from normal
- No anomalies in the vestibular part of the inner ear.
- Bilateral and symmetrical widening of IAC – Bulbous internal auditory canal
- Wide-angle between first and second parts of the intratemporal facial nerve.
- The labyrinthine portion of FN has a more superior position in relation to the cochlea. This part of the nerve will be located almost above the cochlea.
- Cochlear nerve, vestibular nerve, and facial nerves appear normal in MRI.
Management of Hearing loss in IP-III
Rehabilitation depends on the hearing loss level. Hearing aids or Cochlear implants (CI) can be considered in such patients. Cochlear Implant is the best option for hearing in case of IP-III type.
The air-bone (AB) gaps are not significant, and hence no stapes surgery should be done. Also, a stapes surgery in IP-III can lead to CSF gusher and further deterioration of hearing.
Cochlear implantation in IP-III
When considering CI in IP-III, various factors are important.
CSF gusher
A gusher will be invariably present in all persons of IP-III at the time of surgery. Normally, the internal auditory canal (IAC) is separated from the labyrinth at its lateral end by the bony plate of lamina cribrosa. The nerve fibers pierce this bony wall as they come out of IAC. This barrier separates perilymphatic space and subarachnoid space. An abnormal connection between these two spaces may exist in inner ear malformations, leading to CSF gusher. Since the internal auditory canal is ballooned and widely open in incomplete partition type III deformity, profuse CSF gusher will occur in all cases of IP-III cochlea.
Complete control of leak is needed, followed by optional continuous lumbar drainage in the post-operative period. In case of difficult to address CSF leak, a subtotal petrosectomy with blind sac closure of ear can be considered.
Misplacement of the electrode into IAC
Because of the anomalous (ballooned), IAC and absence of modiolus, electrode misplacement into IAC is very common in these patients. An intra-operative trans-orbital X-ray can identify the location of the electrode. If wrongly placed, the electrode needs to be reinserted properly.
Electrode selection in IP-III
- Because of the absent modiolus, Sennaroglu et al recommend the usage of a full banded electrode (with complete rings or contact surface on both sides) as they may provide better stimulation.
But Incesulu et al are of the opinion that a half banded electrode is the best option in IP-III. This is because a full banded electrode can lead to unwanted stimulation of the facial nerve. - Shorter electrodes (25mm) which will make just one turn around the cochlear are preferred because longer ones can fall into the center of the cochlea and can go into IAC.
- Modiolar hugging electrodes are avoided, as the chance of them falling into the cavity is high.
Sennaroglu et al have designed a special type of cork electrode which can be used in these cases. These special electrodes are called FORM electrodes and are manufactured by MED-EL. These electrodes come with a cork type stopper having an outer diameter of 1.9mm. For the 1mm thickness electrode insertion, a cochleostomy is made with a 1.2mm burr. When the electrode is placed, the cork will fit tightly inside the cochleostomy avoiding a CSF leak. These electrodes are also full banded and short ones.
Outcome of cochlear implantation in IP-III
Cochlear implantation in patients with incomplete partition type III can be challenging and thorough knowledge of anatomy is essential. Prior counseling regarding guarded outcome and eventualities are necessary for such patients.
Smeds et al in their study among 10 IP-III patients observed that postoperative electrical stimulation levels were higher in 9 children, as compared with regularly reported average levels in patients with a normal cochlea. 8 children developed spoken language to various degrees. 2 children were still at the pre-communication level. However, speech recognition scores were lower than regular pediatric cochlear implantation cases.
Sennaroglu et al have also reported good outcome for cochlear implantation in IP-III patients. 9 out of 10 children with IP-III malformations of cochlea had a good outcome post cochlear implantation.
References
- Sennaroglu L, Bajin MD. Incomplete partition type III: A rare and difficult cochlear implant surgical indication. Auris Nasus Larynx. 2017 Mar 16. [Epub ahead of print]
- Sennaroglu L, Atay G, Bajin MD. A new cochlear implant electrode with a “cork”-type stopper for inner ear malformations. Auris Nasus Larynx. 2014 Aug 31;41(4):331-6.
- Choi JH, Lee KY, Lim EJ, Lee SH. Cochlear implant in patients with incomplete partition type III. Korean Journal of Otorhinolaryngology-Head and Neck Surgery. 2009 Jun 1;52(6):492-7.
- Smeds H, Wales J, Asp F, Löfkvist U, Falahat B, Anderlid BM, Anmyr L, Karltorp E. X-linked Malformation and Cochlear Implantation. Otology & Neurotology. 2017 Jan 1;38(1):38-46.
- Incesulu A, Adapinar B, Kecik C. Cochlear implantation in cases with incomplete partition type III (X-linked anomaly). European Archives of Oto-Rhino-Laryngology. 2008 Nov 1;265(11):1425-30.